16
THE BULLETIN
and explained to the patient: appropriate acoustic therapy; use of
hearing protection (all patients should wear earplugs or ear muffs
when they are exposed to excessively loud sounds; and strategies
for management of insomnia, anxiety, or depression. As appro-
priate, provide patients with referral and contact information for
physical or psychiatric evaluations, psychological counseling, and
other recommended services or products. A course of cognitive-
behavioral therapy (CBT) is often helpful for patients who experi-
ence anxiety or insomnia, and those who engage in catastrophic
thinking associated with tinnitus.
Acoustic therapy
Patients should add pleasant sounds (music, rain, or waterfall
sounds) to any environment that is too quiet, and listen to them
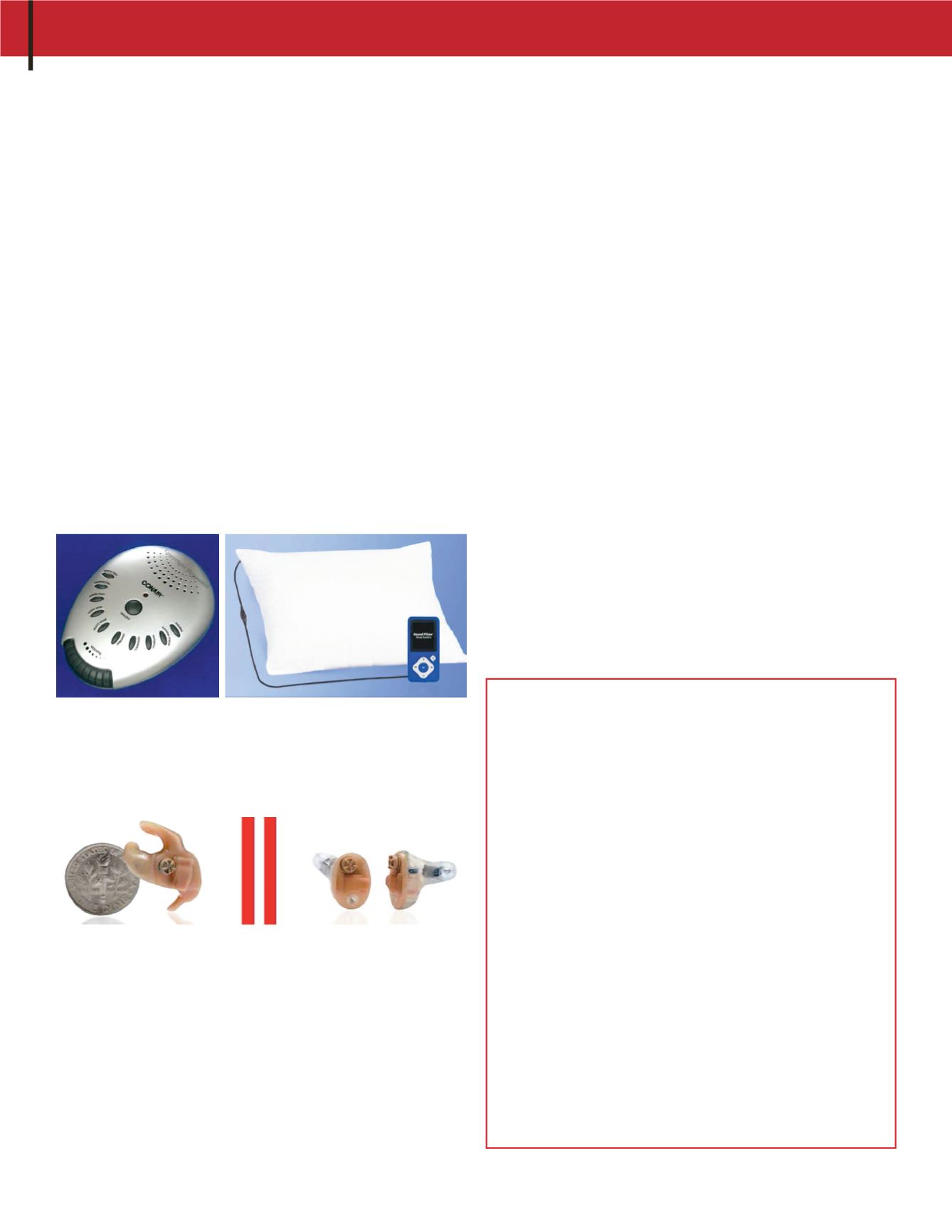
through speakers, headphones, or ear buds. Patients who experi-
ence chronic insomnia because of tinnitus may find relief in using
a tabletop sound machine (or iPhone, iPod) in combination with a
pillow embedded with speakers (such as the Sound Pillow: www.
soundpillow.com).
Patients with normal or nearly normal hearing might benefit
from in-the-ear sound generators (such as those manufactured
by General Hearing Instruments, Harahan, LA) that produce a
broadband sound—similar to water running in the shower—to
muffle or mask the tinnitus.
Significant, aidable hearing loss can often be lessened with
hearing aids or combination instruments (hearing aid and sound
generator in one unit). Hearing aids not only improve patients’
communication ability, the devices can also reduce their percep-
tion of tinnitus immediately and help to reduce tinnitus severity
with sustained use.
10
Experimental treatments for tinnitus
New treatments for tinnitus have been developed and tried for
centuries, and it seems that a new treatment is announced every
REFERENCES
1. Hoffman HJ and Reed GW. Epidemiology of tinnitus. In: J.B. Snow JB (Ed.),
Tinnitus: Theory and Management,
2004:16–41. Lewiston, NY: BC Decker Inc.
2. Henry JA et al. Principles and application of educational counseling used in
progressive audiologic tinnitus management.
Noise Health,
2009;11(42):33–48.
3. Meikle MB et al. The Tinnitus Functional Index: A new clinical measure for
chronic, intrusive tinnitus.
Ear & Hearing,
2012;33(2):153–176.
4. Folmer RL and Griest SE. Tinnitus and insomnia.
Am J of Otolaryngology,
2000;21(5):287–293.
5. Folmer RL et al. Chronic tinnitus as phantom auditory pain.
Otolaryngology–Head and Neck Surgery,
2001;124(4):394–400.
6. Folmer RL et al. Tinnitus severity, loudness and depression.
Otolaryngology–Head and Neck Surgery,
1999; 121:48–51.
7. Folmer RL et al. Obsessive-Compulsiveness in a Population of Tinnitus
Patients.
Int Tinnitus J,
2008;14(2):127–130.
8. Folmer RL. Long-term reductions in tinnitus severity.
BMC Ear Nose and
Throat Disorders,
2002;2:3.
9. Duckro PN. Comprehensive behavioral management of complex tinnitus: a
case illustration.
Biofeedback Self Regul,
1984;9(4):459-469.
10. Folmer RL and Carroll JR. Long-term effectiveness of ear-level devices for
tinnitus.
Otolaryngology–Head and Neck Surgery,
2006;134(1):132–137.
11. Folmer RL et al. Experimental, Controversial and Futuristic Treatments for
Chronic Tinnitus.
JAAA,
2014;25(1):106–125.
12. Folmer RL et al. Repetitive Transcranial Magnetic Stimulation Treatment for
Chronic Tinnitus: A Randomized Clinical Trial.
JAMA Otolaryngology-Head
& Neck Surgery,
2015;141(8):716–722.
week. These have included dietary supplements, antioxidants,
naturopathic concoctions, prescription medications, experimental
drugs, acupuncture, low-level laser therapy, customized sound
therapy, transcranial magnetic stimulation (TMS), transcranial
direct current stimulation (tDCS), vagus nerve stimulation—the
list goes on and on. For a review and critique of many of these
tinnitus treatment strategies, see Folmer et al.
11
While some of
these methods show promise, the majority of them are not effec-
tive for reducing tinnitus perception or severity. Even treatments
that demonstrated efficacy in controlled clinical trials (such as
TMS
12
) require more rigorous vetting via multi-site studies before
they should be implemented clinically. In the meantime, while
the search for the “cure” continues, tinnitus patients and clini-
cians can immediately implement effective management strate-
gies described in this article.
Follow-up
Encourage patients to ask questions about recommended tinnitus
management procedures and to report their progress. Reassess
patients at 1 month. If necessary, recommendations can be modi-
fied to facilitate patient improvement. Follow-up questionnaires
can be mailed to patients 6 and 12 months after their initial
appointment to assess the effectiveness of the tinnitus manage-
ment program
.
TINNITUS, CONT.


